Annals of Bioethics & Clinical Applications
MEDWIN PUBLISHERS ISSN: 2691-5774 Committed to Create Value for Researchers
Is a Medical Vocation Possible Today? Is a Christian Medical Vocation Possible Today?
Pilar Nunez Cubero M1,2*
1Department of Bioethics, Comillas Pontifical University University, Spain 2Department of Philosophy, Ramon Llull University, Spain
*Corresponding author: M Pilar Núñez Cubero, Department of Bioethics, Comillas Pontifical University & Department of Philosophy, Ramon Llull University, Spain, Email: pnunezcubero@ gmail.com
Commentary
Volume 5 Issue 2
Received Date: June 02, 2022 Published Date: June 13, 2022 DOI: 10.23880/abca-16000234
The “Mater Care” Group, which brings together the Obstetricians and Gynecologists of the International Federation of Catholic Medical Associations, was pleased to dedicate its biannual session in 2019 to the analysis of the decision to be a doctor today, wondering if it is still a vocation, as it has always been considered, or has become an attraction to the development and application of new technologies and the management of other values that give more importance to the success of the technique than to the humanization of patient care. It was not in vain that Mgr. Redrado, OSJD wrote: our Hospitals are, today, temples of science and technology, and many times they are not focused on the patients but on other interests, to the point that research seems to go beyond them. The big question that arises is: Should we do everything that science and technology offers us today? Does science have limits? We must do what can best serve people and especially the sick [1].
We have to ask ourselves: if we have not passed from the spirit of the Good Samaritan, to that of a “cyber doctor”, or to that of a transhumanist for whom everything is allowed as long as he manages to eliminate all suffering and achieve a life without death and, if The time has not come to reflect on the need to move from evidence-based medicine to a patient centered medical art, to a totally person-centered medicine.
Current Situation Medicine, Science & Society in the Third Millennium
Years ago every vocation was a call, linked to Christianity, the call of God. Martin Luther and John Calvin emphasized the importance of all work as something to which a person was called by God. There was an idea that everyone’s work – in our case, medicine was a God’s calling.
The characteristics of a call of this type mean that a medical career has less to do with personal fulfillment and more with a response to a need and a requirement to contribute to the common good. A mentality centered on “us” or “Society”, instead of on me, on the SELF.
Thinking of this generation, some believe that today this attitude seems to have been lost… Among students, residents, young doctors, the conversations about Medical Career seem to focus on oneself: How much money am I going to earn? How much prestige am I going to achieve? What lifestyle will I be able to have? Am I going to perform? Some time ago the medical profession has ceased to be a liberal profession to follow an administrative model, even governed by agreement. The issue that worries the most seems to be the “I”. Before, medicine was the means to help people, now it is not. This is tied to a broader sociological environment that emphasizes personal self-actualization and individual autonomy over collective well-being.
Robert Bella in his book (Habits of the Heart) writes: “we have put our own good, as individuals… ahead of the common good.” (“We have put our own good, as individuals… above the common good”) and this is an especially acute problem in medicine, since we are not taking care of people’s finances or products, but rather we are taking care of people in a moment of vulnerability. Medicine is a position where you get money and prestige. It is an easy activity to seek personal gain, but it is a particularly dangerous profession, in which
2 Annals of Bioethics & Clinical Applications
seeking such possibilities can have repercussions and lead to inappropriate care of the vulnerable people to be served.
An upward path is given: When medicine is sought only for personal fulfillment, we see our patients as mere objects rather than people in need. If patients are presented to us as cases that do not bring us interest for our academic careers…, they become annoying, annoying, and we use them without interest, because their questions do not bring us any benefit, unless we can make some publication with their case to enhance the resume. They are patients who are not worth our time. We do not see in them people in need of help, nor do we see ourselves as public servants, rather the patients become a secondary point of interest, even an obstacle to our goals.

If we think like this…We Will Be Doctors, Not Caregivers
If we want a truly caring generation of doctors, we have to change the culture of “me and medicine” to one of “medicine and patients” and our helping role. Bellah wisely says, we have to return to “the idea of medical work as a contribution to the good of all, and not merely as a means to our own progress.”
If today we deeply reconsider the reason for medicine, perhaps we will find in our hearts a genuine desire to always be there for our patients.
Vocation
It will be necessary to establish the difference between PROFESSION and VOCATION
• Profession is a type of job that requires deep, modern training and practical experience or skills. Practice as a professional, really means that one has to do what others think you are capable of doing, with competence, and for that you deserve respect. Depending on the workplace and its type, it can be presented in different ways, and professional work is normally sealed with one form of contract or another.
• Vocation is the occupation to which one strongly feels the need to dedicate oneself, regardless of earning money or other benefits. The personal vocation should be what one feels driven to do because that gives a deep meaning to his life. A type of work that you feel compelled to do and to which you spend most of your time and energy
To work in medicine, one should have a vocation for it. Vocation that implies being “rigorously scientific, deeply human, and ethically correct”, since it is the ideal destiny, the specific mission that each person has to be and to do in their own life, something in us that struggles to be fulfilled and that collides with our environment –soul, body, social world, nature- so that they allow it to “be”, to carry out its mission (Ortega y Gasset). A call to a certain way of existing, what we feel “have to be”, the task or project of existence that must be carried out.
The first sign of personal vocation is LOVE, which fights and overcomes the difficulties against it, which try to keep him from dedicating himself to it and fulfilling his vocation, as the unavoidable personal task.
Medical Vocation
The Medical Vocation supposes that inner desire and that love against all difficulties, since it needs all levels of interpretation (literal, moral, allegorical, and analogical) to achieve a true DOCTOR-PATIENT ENCOUNTER.
In the first meeting, the doctor has to evaluate the patient’s situation, the plausibility of his terms, the inaccuracies in his expression and the narrative fidelity, for the benefit of the patient and to create empathy. And at the same time explore the patient’s values. Without forgetting that the human person is a unit, not a conglomerate of 5 components

After the first meeting, he has to follow the path of reason to get to know the truth: the reality of the patient in the physical, mental, social, spiritual and emotional (Zubiri), always confronted with a system of references , to point out some possibilities of diagnosis and differential diagnosis and checking the veracity of these possibilities (evidence)
3 Annals of Bioethics & Clinical Applications
And after that, come to the path of morality to contrast if there are some values in conflict and if there were, respecting personal autonomy, allowing the patient to participate in deliberation and decision “without forgetting that an emotional situation can lead the patient to an axiological blindness” and that it will be necessary to give him time to deliberate and arrive at the correct decision.
Physicians, in the exercise of their profession, cannot forget their moral principles, neither at the time of their medical acts, nor at the time of manifesting them. Their bioethical training should not be based only on Principles, but also and, mainly, on the virtues, especially prudence, not as caution but as Phronesis or practical wisdom (Pellegrino), keeping in mind a great sense of duty, since often it is well known what can be done, but what one has the DUTY to do is ignored.
The autonomy of the patient requires respect, but not discharging all responsibility on him, as a moral, autonomous and responsible subject must be included in the process of deliberation and decision-making in everything that concerns him. It will be necessary to jointly analyze the facts, reflecting on the values that are at stake, to deduce the duties to be followed:

The moral conscience has to guide and give an orientation on the moral decision. It is about a type of conscience that can guide us in the most difficult decisions because it in the subjectivity of DUTY, where ethical decisions have to be made, knows that Medicine is a science of probability and not a science of certainty, and without forget that all moral conscience is manipulable.
The Legislation and the Codes of Medical Ethics have to incorporate the conscientious objection of doctors for ethical, moral and religious reasons, in order to guarantee the freedom and independence of professionals, without neglecting to consider that there are pathological consciences due to laxity or because of their rigidity, and without forgetting that Conscientious Objection is PERSONAL.
The Medical Vocation Today Asks
Love for medical work, Love for the patient, Competence, Dedication and so when what one wants to do and what one must do coincide, peace and joy are produced: “you enjoy with and in medical work”.
The Christian Medical Vocation is identified with the image-model of the Good Samaritan

Vocation of the Christian Lay Physician, and of Catholic Health Personnel
He asks “to see daily tasks as an opportunity to get closer to God, to fulfill his will, and to serve others by bringing them closer to God.” Christifideles Laici 52 and giving a coherent testimony of it with life. “A baptized Christian who is truly baptized in his heart, living and fulfilling his profession wherever in the world he lives and exercises his profession, can be a true Christian.”
Christifideles Laici invites the following fields of action: • Promote the dignity of the person;
• Protect the inviolable right to life;
• Recognize religious and family freedom in their social environment;
• Act with Charity as inspiration and support for solidarity; • Accept the duty of every person to express themselves in politics;
• Consider the centrality of the person in the social and economic sphere;
• And evangelize the culture both at a general level and each culture in particular.
• The Pope, Francisco, thus addressed health workers “treat the sick as a person, not as a number” (June, 2019). • Take care of the defense, respect and promotion of life. • The health system and treatments have changed radically, not only due to technological advances, but also because more serious problems of an ethical nature have appeared.
• Any medical practice or intervention on the human being must be carefully evaluated on whether it respects life and human dignity.
• Appreciates the “irreplaceable service” to the most vulnerable or most needy people based on illness, age or marginalization.
Look at your patient; learn to call him by name. Be open to the unpredictable”.
4 Annals of Bioethics & Clinical Applications
Each person is unique and unrepeatable; contemplating the humanity of Christ teaches us that every individual is not a number, but a person, unique and unrepeatable”. The efficiency of the Corporation and the reduction of costs often put the needs of the patient in second place, rather than accompanying them throughout their illness.
Christian professionals are encouraged to devote particular attention to spirituality. So that this fundamental dimension of the person, so important but often forgotten in our time, is once again valued and appreciated, especially for those who live with the disease and for all those who are close to those who suffer”.
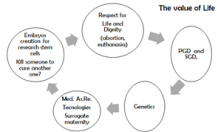
CHALLENGES posed to the medical vocation, Christian or not, by Modern Medicine and Contemporary Society. The challenges of modern medicine and society to the medical vocation focus on the value of life and human dignity from beginning to end (abortion, euthanasia…)
• Consider the value and application of Prenatal Genetic Diagnosis or PGD and Systematic or Screening Diagnosis, SGD, when authors, such as Savulescu, claim that parents have a moral obligation to perform Genetic Diagnosis of their embryos and make a selection of the embryos. Themselves.
• The creation of embryos for the purposes of reproduction, research or treatment.
• Cloning to obtain stem cells. You cannot eliminate a life to save another life.
• Assisted reproduction, up to what limits… Up to surrogacy?
• Transhumanist and post humanism (can and should man be changed?)
• The robotic. Can robots and cyborgs treat and care for the patient?
• The Society of maximum well-being, the greatest well being, for whom? For everyone?
• Gender situations, for whom? Why?
• Ethics, Law, Legislation and Policy
Transhumanist, why and for whom? There is a difference between trying, improving and wanting to change man

Gender Situations and Theories: Queer Theories… The greatest possible Well-being, physical, intellectual, social, emotional, spiritual, economic, occupational, environmental… For whom? For each and every one?
The Autonomy of the Patient, can the patient demand a treatment that is not medically indicated? Change from a Paternalistic Medicine to an Autonomist or Deliberative Model.
Bureaucracy a New World Order
• A techno-liberal globalization
• A technical globalization of the community • Genetics and germ line therapy
• The Hybridization “Machine-Man” (Cyborg) • Artificial Intelligence (not different from Humans) Kurzweil
• Converging Technologies: NBIC
• Transhumanism and Posthumanism
• A New Humanity (Avatar 2045)
Politicization & Commercialization the 4th Industrial Revolution.
Ethics and Law “Legislation”
Ethics
Do we have to do everything that science and technology offer us?. What should we do…? What is necessary to serve people, the sick? LAW: Can the Law compel the withdrawal of a treatment and lead the patient to his death?.
Is it possible to legislate to impose the “Reproductive Right” including the end of a pregnancy?
5 Annals of Bioethics & Clinical Applications
Conscientious objection is based “on the personal need not to act against one’s own ethical conviction”
The choice to object must be made with respect and humility, without becoming a reason for pride or vanity. In these situations, it is essential to exchange reasons and dialogue “especially with those who hold different positions”, always avoiding condemnation. Today it seems that our hospitals are temples of science and technology, and they are not focused on the sick, even in some cases the research goes beyond the individuals… the sick. The doctor will often have to remain in a democratic disagreement, remaining in conscientious objection when many of the decisions go against our values, and against a Christian vision of man and life.
The demand for coherence about life could lead, in extreme cases, to the greatest and supreme testimony of martyrdom, as the martyrs of the 19th century in Korea show us…, and now, it can lead us to lose our jobs.
Conclusion
Is Medicine a possible vocation today? Yes, it is always possible to heal and care for the people who live in our world, real people and Cyborgs. Serving the most vulnerable… the poor, the refugees, the homeless, as well as those living in developing countries, the least advantaged You will always have the poor with you, and whenever you have a desire you can do them good, (Mk 14, 7)
Annexes
Full text of the Geneva Declaration, October 2017 Physician’s Promise
• I SOLEMNLY PROMISE to dedicate my life to the service of humanity;
• ENSURE above all for the health and well-being of my patient;
• RESPECT the autonomy and dignity of my patient; • MONITORING with the utmost respect for human life; • DO NOT ALLOW considerations of age, illness or
disability, creed, ethnic origin, gender, nationality, political affiliation, race, sexual orientation, social class… to come between my duties and my patient;
• KEEP AND RESPECT the secrets entrusted to me, even after the death of the patient;
• EXERCISE my profession conscientiously and with dignity and in accordance with good medical practice; • PROMOTE the honor and noble traditions of the medical profession;
• GIVE my teachers, colleagues, and students the respect and gratitude they deserve;
• SHARE my medical knowledge for the benefit of the
patient and the advancement of health;
• TAKE CARE of my own health, well-being, and abilities to provide health care of the highest standard;
• NOT TO USE my medical knowledge to violate human rights and civil liberties, even under threat. I MAKE THESE PROMISES solemnly and freely, under my word of honor.
A Code or Constitutional Charter for Physicians: Professionalism
Rev Chile Infect 2004; 21(1): In February 2002, a very interesting document was published simultaneously in the Lancet1 and Annals of Internal Medicine 2 journals. It is the proposal for a new Code or Constitutional Charter for the medical profession, which proposes the ideals to which “all medical professionals can and should aspire [1].” The document is the product of several years of joint work by three very important institutions dedicated to internal medicine and, to a large extent, regulating it: the American Board of Internal Medicine, the American College of Physicians and the European Federation of Internal Medicine. Despite this origin, its scope reaches all medical disciplines. The Code consists of an introduction or preamble of its foundations [2], followed by the proposal of three basic principles and ten commitments.
Preamble
Professionalism is the basis of medicine’s contract with society.
The word “professionalism” in the Spanish language does not reflect the content of that Constitutional Charter, but it is universally accepted, probably because in English it better expresses the content of this document. In any case, this Charter or Code establishes principles and commitments that are specific and exclusive to the medical profession. All doctors should know the content of this Code and try to put it into practice. Medical journals, specialty societies, and medical schools should be involved in the effort to spread these ideas [3-6].
Fundamental Principles
• Principle of Primacy of the Welfare of the Patient: Altruism contributes to trust and a good doctor patient relationship. Market forces, social pressures and administrative requirements cannot violate this principle.
• Principle of Patient Autonomy: Physicians must be honest with patients and empower them to make informed decisions about their treatment.
• Principle of Social Justice: Physicians must actively work to eliminate all discrimination in health care,
6 Annals of Bioethics & Clinical Applications
whether for reasons of ethnic or racial, gender, socioeconomic, religious or any other social category.
Professional Responsibilities or Commitments
• Commitment to Professional Competence: Doctors must learn all their lives.
• Commitment to Professional Competence: Physicians must learn a lifelong commitment to honesty with patients. Physicians must ensure that patients are fully and honestly informed before agreeing to treatment; should be able to decide on the course of therapy.
• Commitment to Maintaining Appropriate Relationships with Patients: Physicians should never take sexual advantage of their patients, obtain personal financial gain from them, or use them for any other private purpose.
• Commitment to Patient Confidentiality: Satisfying the commitment to confidentiality is more important today than ever before, given the widespread use of electronic information systems to collect patient data.
• Commitment to a Better Quality of Care: The doctor must work with other professionals to reduce errors, increase patient safety, avoid excessive use of resources and optimize health care.
• Commitment to Improving Access to Care: Physicians must individually and collectively strive to reduce barriers to equitable health care.
• Commitment to a Fair Distribution of Limited Resources: Physicians must commit to working with other physicians, hospitals, and economists to develop cost-effective care guidelines. The professional responsibility of physicians for an appropriate allocation of resources requires scrupulously avoiding superfluous tests and procedures.
• Commitment to Maintain Trust in the Face of Conflicts of Interest: Physicians have an obligation to recognize, alert the general public, and deal with conflicts of interest. Relations between the industry and opinion leaders must be transparent.
• Commitment to Scientific Knowledge: Physicians have a duty to safeguard scientific standards, promote research and create new knowledge, ensuring its proper use.
• Commitment to Professional Responsibilities. Physicians are expected to participate in self-regulatory processes, including rectifying and disciplining members who have failed to meet professional standards.
References
1. (2002) Medical Professionalism in the new millennium: a physicians’ charter. The Lancet 359(9305): 520-522.
2. ABIM Foundation, ACP-ASIM Foundation, European Federation of Internal Medicine (2022) Medical professionalism in the new Millennium: a Physician Charter. Ann Intern Med 136(3): 243-246.
3. Blank L, Kimball H, McDonald W, Merino J (2003) Medical professionalism in the new Millennium: a Physician Charter 15 Months Later. Ann Intern Med 138(10): 839- 841.
4. In short, the practice of medicine in the modern era is subject to great real or virtual challenges, in all cultures and societies.
5. These challenges center on increasing inequalities between the legitimate needs of patients, the resources available to meet those needs, the increased reliance on market forces to transform health systems, and the temptation of healthcare professionals to forget their traditional commitment, the priority of the patient’s interests
6. To maintain fidelity to the social contract during this turbulent time, physicians need to reaffirm their active dedication to the principles of professionalism, which requires not only a personal commitment to the well
being of their patients, but also a collective effort to improve healthcare systems. Health for the good of society.